The anal glands—approximately 6-14 of them—run along the anal canal. When these glands become clogged or infected for any reason, such as frequent bowel movement, constipation, or frequent diarrhea, or due to a blockage from fecal or foreign matter, this can cause a perianal abscess.
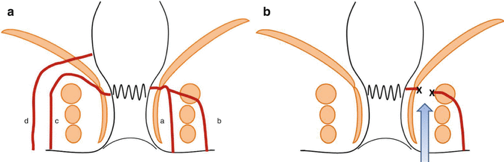
If treatment of a perianal abscess is delayed the abscess can break outward through the skin in the anal area (point D in the image) and can result in a chronic fistula-in-ano (points 1, 2, 3, 4 in the image). Even with treatment, however, there is still a 10-50% chance of developing a fistula-in-ano, depending on the physical condition of the individual. The anal anatomy is complex, and so the symptoms of perianal abscesses and fistula-in-ano can be different for each individual patient. It is important, therefore, not to delay, but to receive diagnosis and treatment from a colorectal surgery specialist as quickly as possible for best results.